Karma Ugyen1, Nima Dema1, Damcho Wangchuk2, Sangay Thinley3, Tempa Gyeltshen4
![]() , Sherab
Tenzin 5, Karma Tenzin6
, Sherab
Tenzin 5, Karma Tenzin6![]()
1National Traditional Medicine Hospital, Thimphu, Bhutan
2Traditional Medicine Unit, Wangdicholing Hospital, Bumthang, Bhutan
3Traditional Medicine Unit, Eastern Regional Referral Hospital, Mongar, Bhutan
4Faculty of Traditional Medicine, Khesar Gyalpo University of Medical Sciences of Bhutan, Thimphu, Bhutan
5Menjong Sorig Pharmaceuticals, Thimphu, Bhutan
6Faculty of Postgraduate Medicine, Khesar Gyalpo University of Medical Sciences of Bhutan, Thimphu, Bhutan
Corresponding author: Karma Ugyen, National Traditional Medicine Hospital, Thimphu, Bhutan.
Email: ugyensangay@gmail.com
DOI: https://doi.org/10.47811/bsj.0013050815
Copyright © 2025 Bhutan Sorig Journal published by the Faculty of Traditional Medicine, Khesar Gyalpo University of Medical Sciences of Bhutan.
This is an open access article under the CC BY-NC-ND license.
ABSTRACT
Introduction: Urine reflects the body’s functional status playing a central role in the diagnosis of disease conditions. This study aimed to compare six of the nine features of urine at physiological and lukewarm states after artificial heating – colour, odour, steam, bubbles, sediment, and frothiness.
Method: This comparative study utilized the Bhutan Analysis System for Urine Properties (BASUP) chart. The study was conducted from July 2021 to January 2022 at the Eastern Regional Referral Hospital, Wangdicholing District Hospital, and the National Traditional Medicine Hospital. The properties of urine were evaluated soon after collection at physiological state. After the urine specimen had cooled down to room temperature, it was heated to body temperature following a standard procedure for reassessment of its properties.
Results: A total of 91 specimens from 35 men and 56 women were analysed. There were no significant differences observed in the colour, odour, steam, bubbles, sediment, or frothiness between physiological and artificially heated specimens. However, there were differences in the colours of དམར་ཤས་ཆེ་བ། (Marshechewa) with p = 0.023 and སེར་ཤས་ཆེ་བ། (Sershechewa) with p = 0.015.
Conclusions: The study found no significant differences in the majority of the properties of urine in specimens at physiological state and after artificial heating. However, further studies are required to evaluate the physicochemical properties and the differences in the Marshechewa and Sershechewa colours noted.
Key words: Diagnosis; Traditional Medicine; Observation; Urinalysis; Urinary Sediment Analysis
INTRODUCTION
Traditional Medicine (TM), known as Sowa Rigpa, holds that the human body consists of three primary elements: rLung (Air), mKhris-pa (Bile), and Bad-kan (Phlegm). A state of health is achieved when these elements are in harmonious balance within the body [1]. In TM, the primary diagnostic techniques are pulse reading and urine analysis. Urine reflects the body’s metabolism and the functional status of various organ systems [2].
In Sowa Rigpa, urine analysis is regarded as the most distinctive and effective diagnostic method due to the extensive clinical information it provides. There are nine clinical features assessed at three different temperature states. Historically, urine analysis at the National Traditional Medicine Hospital (NTMH) was performed on cold samples, which is different from the natural physiological state at body temperature. At the NTMH, this method was officially adopted in 2014 following thorough deliberations among traditional medicine practitioners. The practice of heating urine for analysis was first introduced by Sangay Gyatso (1652 – 1705) in Tibet [3, 4].
Urine is analysed at three temperature stages: body temperature, lukewarm, and cold stages. Soon after evacuation from the bladder at body temperature, the urine specimen is evaluated for colour, vapour, odour, and bubbles. At the lukewarm stage, the specimen is evaluated for frothiness and sediments. In the cold stage, the timing and pattern of colour changes, along with the clarity or cloudiness of the fluid after transformation are recorded (Figure 1) [5]. The location of sediments in the tube indicates the location of the disease in the body (Figure 2). Sediments at the upper part of the test tube suggest symptoms like dizziness, heart, or lungs-related issues; sediments at the middle part of the test tube suggest indicate liver or spleen-related disorders; and sediments at the lower part of the test tube point to colon, intestine, kidney and bladder issues, lower body rlung problems, or diarrhoea [6].


The characterization of the colour of the specimen was compared to the standard template from the Bhutan Analysis System for Urine Properties (BASUP) chart 2021. (Figure 3) was developed through expert consultation among Traditional Medicine experts at the NTMH, Thimphu, Bhutan. As per Sowa Rigpa text, it is preferred that the characteristics of urine specimens are assessed at physiological state [7]. However, this method is often not feasible owing to patient timing for hospital visit. Thus, it is important to determine whether the characteristics of artificially heated urine specimens are comparable to those from specimens in their natural physiological state. Therefore, the objective of this study was to compare the characteristics of artificially heated urine specimens with that of characteristics as physiological state.

Study Design
This was an observational study. In this study, the following selected characteristics were compared with urine specimens analysed at physiological state (soon after evacuation) and after artificial reheating to body temperature: colour, vapour, odour, bubbles, sediment and frothiness.
Study site
This study was conducted at the National Traditional Medicine Hospital, Thimphu; Eastern Regional Referral Hospital, Mongar; and Wangdicholing Hospital, Bumthang between July 2021 and January 2022.
Study population, sample size and sampling method
All patients visiting the selected hospitals, irrespective of their diagnoses, were invited to participate in the study. The patients were provided advices on dietary restrictions (avoidance strong tea, butter milk, alcohol and milk) and behaviour restrictions (avoidance of dehydration, sleep deprivation, sexual activities, mental stress, and excessive physical activity) as per the Sowa Rigpa text until specimen collection [8]. All patients who consented and reported to the hospital to provide their specimens were included.
Urine specimen collection and handling
The flow of patients involving screening, collection and analysis of urine specimens is shown in Figure 4. Among the nine clinical features of urine, three related to cold-state specimens were excluded, as the study focused on comparing artificially heated urine with its physiological state.

Assessment of urine properties at physiological state
Step 1
A sterile container was handed over to the patient to collect about 40 mL of mid-stream urine. This specimen was handed over within one minute to the TM physician and the urine characteristics at physiological and warm states (vapour and odour) were recorded.
Step 2
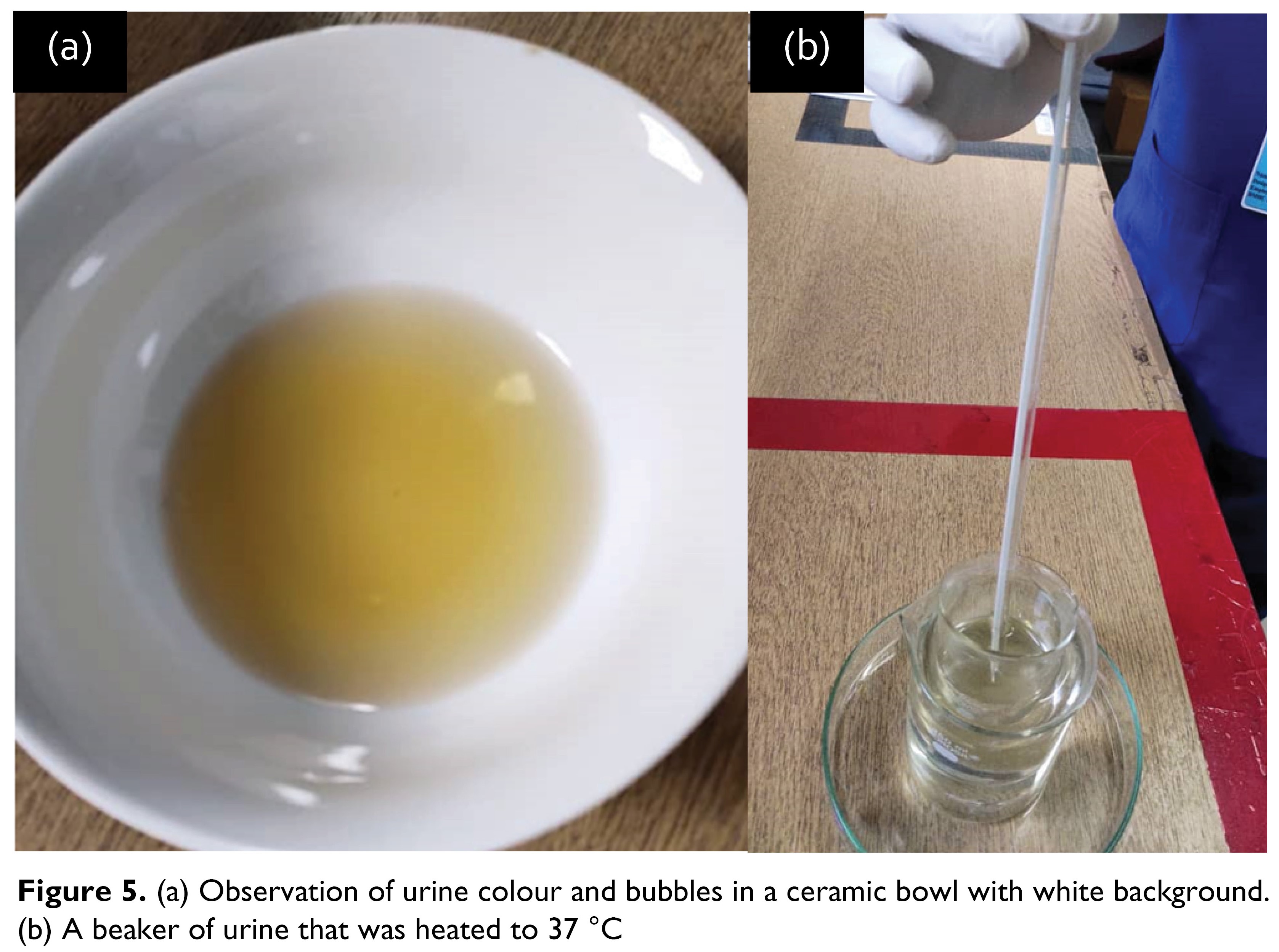
From this specimen, 30 mL of the specimen was transferred into a ceramic bowl (Figure 5a ) to assess colour and bubbles, and the remaining 10 mL of urine was transferred into a test tube and allowed to settle sediments for 20 minutes.
Step 3
Urine characteristics at a lukewarm stage were recorded: sediments and frothiness. Following this, the specimen was left still at room temperature for 20 minutes and the position of the sediments (upper, lower or bottom layer) in the test tube was recorded.
Assessment of urine properties after artificial heating
Step 4
The specimen from the ceramic bowl and test tube was transferred into a beaker with a thermometer, and was then immersed in a jar containing hot water when the temperature of the specimen reached 37 °C (Figure 5b), the contents were poured back into the ceramic bowl to assess colour, bubbles and odour.
The procedure for assessment of urine characteristics after artificially re-heading is described in the Standard Operating Procedure adopted by the NTMH, 2014 [9]. The template for reporting the urine characteristics after artificial heating is shown in Figure 6.

The data on the characteristics of urine specimens were recorded in a pro forma that was designed for the purpose for this study. The TM physicians at all the three participating sites were trained through a workshop on the use of the pro forma and the use of BASUP chart.
Data analysisThe data was double entered and validated using EpiData Version 3.1 (EpiData Association, Odense, Denmark). STATA version 13 (licenced Khesar Gyalpo University of Medical Sciences of Bhutan) was used for analysis. The comparison of the six characteristics were made using chi squared test. P values < 0.05 to as considered significant.
Ethics considerationsEthics approval for this study was obtained from Research Ethical Board of Health, Ministry of Health, Royal Government of Bhutan (REBH/approval/ 2020/10053). Administrative clearance was obtained from the Policy and Planning Division, Ministry of Health and from the respective Medical Superintendents of the hospitals. Informed consent was taken from the study participants prior to specimen collection.
RESULTSThere were 91 urine specimens examined: 29 at NTMH and 31 each at Wangdicholing Hospital and Eastern Regional Referral Hospital. These specimens were from 35 male and 56 female participants.
The details of comparison of colour, odour, steam and bubbles is shown in Table 1. In the comparison of urine colour, there were no differences in སྔོ་བ། (Ngowa), དཀར། (Kar), སེར། (Ser), སྔོ་སེར། (Ngoser) , སྔོ་སྐྱ། (Ngocha), དམར་སེར། (Marser), སྔོ་དཀར། (Ngokar) and others such as སེར་སྐྱ། སྔོ་དམར། རྒྱ་ཤེལ། དཀར་སེར། དམར་སྐྱ། དམར། དམར་ནག. However, there were significant differences in the colours of དམར་ཤས་ཆེ་བ། (Marshechewa) with p = 0.023 and སེར་ཤས་ཆེ་བ། (Sershechewa) with p = 0.015.

In the comparison of urine odour, there were no differences in དྲི་ཆེ་བ། (Drechewa), དྲི་ཆུང་བ། (Drechungwa) and other odours གསུར་དྲི། and ཟས་དྲི། .
In the comparison of steam, there were no differences in རླངས་ཆེ། (Langchewa), རླངས་ཆུང་། (Langchungwa) and other forms of steam རེས་ཆེ་རེས་ཆུང་། and ཡུན་ཐུང་།.
In the comparison of bubbles, there were no differences in སྔོ་ལ་ཆེ་བ། (Ngolachewa), ཕྲ་སེར་སངས་སྐྱེན། (Thrasersangken), མཆིལ་མ་འདྲ་བ། (Chelmadrawa), འཇའ་ཚོན་འདྲ་བ། (Jatshendrawa), ཚེག་སྒྲ་ཡལ་བ། (Tsheg Dra Yelwa), བརྟན་པ། (Tenpa), རྒོད་པ། (Goepa), གསོག་བརྟན། (Sog Ten) and ཡལ་བུལ་བ། (Yel Bulwa).
The details of comparison of trema and sediments is shown in Table 2. In the comparison of trema, there were no differences in སྲབ་པ། (Sapa), མཐུག་པ། (Thukpa), བླངས་བཞག། (Langzha) and དུམ་བུར་ཆད་པ། (Domburchewa). In the comparison of sediments, there were no difference in སྤུ་རྩེ་འདྲ་བ། (Putse-drawa), སྤྲིན་འདྲ་བ། (Tren-drawa), བྱེ་མ་འདྲ་བ། (Jema-drawa), མཐུག་པ། (Thukpa), གསུམ་ག་ཁྱབ་པ། (Sumgacham), བར་གནས་། (Barnepa), འོག་གནས། (Wognepa), ཞོ་ཤི་འདྲ་བ། (Zhoshedrawa), སྲབ་པ། (Sapa), སྤུ་འདྲ་བ། (Pudrawa) and བལ་འདབ་ཆུ་སྐྱུར། (Baldap chuchur).

DISCUSSION
This study demonstrates that the majority of the characteristics of urine specimens artificially heated to body temperature were similar to that at physiological state. This study was done to assess if artificial heating of urine specimens had any untoward alteration of its characteristics. The findings from this study support the practice of artificial heating of urine specimens aligning with the methodology utilized by Sangay Gyamtsho [10].
The comparison between physiological and artificially heated urine samples showed that most cloudiness and sediment characteristics remain consistent across both methods. The thick and thin sediments in urine play a crucial role in disease diagnosis was said by Yothok Yoenten Gonpo, “ཆུ་མ་ངེས་ཇི་ལྟར་འདུག་ཀྱང་རུང་། །ཀུ་ཡ་མཐུག་ན་ཚ་བ་དང་། །ཀུ་ཡ་སྲབ་ན་གྲང་བ་ཡིན། ། In addition to the eight clinical characteristics, the key factor in analysis of urine is the sediment.” According to his teaching, thick sediments in the urine point to heat-related diseases, while thin sediments indicate cold-related conditions [4, 11].
No significant disparities were detected across all parameters concerning frothiness and sediments between the two methods. This finding aligns with the statement “ངད་ཡལ་དུས་སུ་ཀུ་ཡ་སྤྲིས་མ་བརྟག” which describes that frothiness and sediments are typically observed in the lukewarm stage, where temperature variation is minimal across both urine samples [12].
According to the Subsequent Tantra, the presence of thick and thin concentration frothiness layers on the urine surface suggests hot and cold disorders, respectively [13]. Among the five frothiness specimens analysed, there was no turnover observed in the “Trema thukpa/Very thick frothiness” and “Tremen/ No frothiness” categories. This lack of turnover indicates that there were no extreme patterns of hot and cold conditions among the participants in this study. The Sowa Rigpa phrase “སྤྲིས་མ་སྲབ་ན་གྲང་བ་ཐུག་ན་ཚ” highlights the connection between urine frothiness and the body’s internal heat. Thick frothiness in the urine suggests an excess of heat in the body, which causes the body’s fat to melt and appear as oil-like froth in the urine [14]. On the other hand, a lack of frothiness indicates a cold-related condition that reduces the body’s inner heat, leading to froth-free urine[15].
Anecdotal evidence also suggests that the lack of frothiness in urine nowadays may be attributed to people consuming less oil in their diets. Tumours can also be diagnosed through the observation of urine frothiness. If cracks are seen within the froth, it may indicate the presence of a tumour. Additionally, a tumour can be suspected if small, fish-eye-like bubbles are observed in the middle of the urine specimen [16].
In Sowa Rigpa, patients are advised to follow specific dietary and behavioural restrictions the day before providing a urine sample. This may be a potential influence on the content of the urine specimen and its properties. Further chemical analysis of the impact of dietary and behavioural restrictions on urine specimens is recommended to be studied.
This study is the first of its kind conducted in the country. This study standardizes the use of BASUP chart 2021 in the assessment of colour or urine specimens. However, the primary limitation of the study is all the nine parameters of the urine characteristics in the physiological stage could not be compared in an artificially heated stage. Future studies may be done in larger sample sizes with additional assessment of physicochemical characteristics to further substantiate these findings.
CONCLUSIONUrine characteristics of colour, odour, steam, bubbles, sediment, and frothiness were consistent between urine samples in the physiological state and those subjected to artificial heating. However, there were differences in colour of དམར་ཤས་ཆེ་བ། (Marshechewa) and སེར་ཤས་ཆེ་བ། (Sershechewa) in the two methods of analyses. Future studies in larger sample sizes and detailed physicochemical characterization of urine specimens are recommended.
Acknowledgement
We express our deepest gratitude to Dorji Gyeltshen, Dhendup Wangyal, and Jambay Dorji of the Sorig Research and Development Division, erstwhile Department of Traditional Medicine Services, Ministry of Health, for their support and training assistance. We also extend heartfelt thanks to Phillip Erbele, Assistant Professor at the Faculty of Nursing and Public Health, Khesar Gyalpo University of Medical Sciences of Bhutan and Tshewang Gyeltshen for their valuable initial review; Tshering Choeda for data analysis and data interpretation and Phuntsho Wangdi for the help in initial development of the study protocol. Our special gratitude goes to Thinley Dorji for his contribution in making revisions to this manuscript
Declarations
Ethics approval and consent to participate.
Ethics approval for the study was obtained from Research Ethical Board of Health, Ministry of Health, Royal Government of Bhutan (REBH/approval/ 2020/10053). Administrative clearance was obtained from the Policy and Planning Division, Ministry of Health and from the respective Medical Superintendents of the hospitals. Informed consent was taken from the study participants prior to specimen collection.
Consent for publication
Not applicable
Competing interests
KU, TG, S Tenzin and KT are members of the editorial board of this journal. They were blinded during the peer review process of this article.
Funding
There was no funding for this study.
Availability of data materials
The dataset is available from the corresponding author upon reasonable request.
Author contributions
Conceptualization, Methodology, Formal analysis, Investigation, Resource: ND, DW, S Thinley, TG, S Tenzin, KT
Writing - Original Draft, Writing - Review & Editing: KU, TG
Formal analysis, Investigation, Data Curation: DW, S Tenzin
Methodology, Resources, Supervision: TG, S Tenzin, KT
Received: 25 Jan, 2024 Accepted: 17 October, 2024 Published online: 11 November, 2024
References
- Wangchuk P, Wangchuk D, Aagaard-Hansen J. Traditional Bhutanese medicine (gSo-BA Rig-PA): an integrated part of the formal health care services. Southeast Asian J Trop Med Public Health. 2007;38: 161–167
- Callens AJ, Bartges JW. Urinalysis. Vet Clin North Am Small Anim Pract. 2015;45: 621–637. doi: 10.1016/j.cvsm.2015.02.001
- རྟེན་འབྲེལ་དབང་འདུས། སངས་རྒྱས་དབང་འདུས། གསོ་རིག་འབྱུང་ཁུངས་མུ་ཏིག་འཕྲེང་མཛེས། ཐོན་རིམ་དང་པ། རྒྱལ་ཡོངས་ནང་པའི་གསོ་རིག་དཔལ་ཁང་། ནང་པའི་གསོ་རིག་འཛིན་སྐྱོང་ལྟེ་བ། ཐིིམ་ཕུག། ༢༠༠༤།
- ཟླ་བ་ཚེ་རིང་། བརྟག་པ་རྩ་ཆུའི་རྒྱས་སྤྲོས་གོ་དོན་རེག་མཐོང་ཡིད་ཀྱི་མེ་ལོང་། མི་རིགས་དཔེ་སྐྲུན་ཁང་། ༡༩༩༧།
- Goenpo C. Chakdor Sorig Chodrek. Dukar, Gytsho P, Traba, Chap K, Tshering L, Tsho R, Dorji, Dorji DR, editor. Tshongoyen Zhingchen, Tibetan Research center, Merig-Petren-Khang; 2005. 443.
- Choedra DL. Lekshey-Sergi-Thurma. Tshering L, Dukar, Tsho R, Traba, Dorji DR, editor. Tibet: Merig-Petruen-Khang; 2004. 251.
- ཐུབ་བསྟན་ལེགས་པའི་བློ་གྲོ ོས། བརྟག་པ་རྩ་ཆུ་ཟུང་གི་འབྲུ་འགྲེལ། རྒྱལ་ཡོངས་ནང་པའི་གསོ་རིག་དཔལ་ཁང་། ཐིིམ་ཕུག ༢༠༠༩།
- སྐྱེམ་པ་ཚེ་དབང་། སྐྱེམ་འགྲེལ། དེབ་༣ པ། ཐོན་རིམ་གསུམ་པ། སྨན་རྩིས་ཁང་། རྡ་རམ་ས་ལ། རྒྱ་གར།
- National Traditional Medicine Hospital. Standard Operating Procedure for Urine Analysis. Thimphu: Ministry of Health, Royal Government of Bhutan; 2024.
- Tshering D. Takpa Tsa-chuyi gaytre Godok Rekthong Nyki Melong. Merig-Petren-Khang; 1997. 137–138.
- ལྷུན་གྲུབ་བཀྲ་ཤིས། དར་མོ། གཡུ་ཐོག་གསར་རྙིང་གི་རྣམ་ཐར་བཞུགས་སོ། བོད། མི་རིགས་དཔེ་བསྐྲུན་ཁང་། ༢༠༠༤།
- དཔལ་སྤུངས་རིག་གནས་མཐོ་སློབ་དོན་གཉིས་ནོར་བུའི་དགའ་ཚལ། གསོ་བ་རིག་པའི་རྒྱུད་སྡེ་རྣམ་བཞི་ལས་རྩ་བཤད་ཕྱི་མའི་རྒྱུད་སྡེ་སྐོར་གསུམ། དཔལ་སྤུངས་མཐོ་སློབ་ལྷན་ཚོགས , editor. Himachal Pradesh India: Pelpung-Sungrab-Partrun-Khang; 2012. 149.
- Tshenam T. Gso rig rgyud bzhi’i’ grel chen drang srong zhal lung Vol 4. Tibet: Merig-Petren-Khang; 2000.
- Mepham. Jumepham-Tsado Trika. Tibet: Merig-Petren-Khang; 1987
- Bum T. Jue-Zhi Kadrel. 1st ed. Hemachal Pradesh H.P: Palpung-Sungrab-Nyamso-Khang; 2008. 434.
- Skrajnowska D, Bobrowska-Korczak B. The Effects of Diet, Dietary Supplements, Drugs and Exercise on Physical, Diagnostic Values of Urine Characteristics. Nutrients. 2024;16: 3141. doi: 10.3390/nu16183141